The COVID-19 pandemic has claimed more than 2.5 million lives worldwide as of today. The case mortality rate (CFR) is an important parameter in COVID-19 mortality research and is defined as the ratio of the number of infectious cases to the death tax number.
CFR serves as a quantitative metric for the severity or lethality of COVID-19 infection. It can be a reference for comparison with other infectious diseases such as Ebola or severe respiratory syndrome (SARS). An urgent application of CFR is to determine the number of infectious cases through the death tolls, as the death toll is believed to be relatively reliable.
CFR is also useful as a proxy for risk assessment.
Understanding factors that contribute to CFR is crucial to the proper execution of CFR. While it is clear that the death of COVID-19 is closely linked to the patient’s health conditions or status, CFR is not sufficient to understand the population at the population or national level. COVID-19 mortality is often the result of other diseases of a person’s lung or heart, which makes it challenging to differentiate CFR at the population level. The CFR observed may vary for different numbers because different methods of mortality in different locations may affect the death toll, the difficulty in determining the true cause of death when comorbidities are present, and also because of numbers lost in reported deaths.
Although CFR has been applied as a measure of infection depth, susceptibility estimates, and risk assessment, there is a lack of understanding of various aspects of CFR. A better understanding of CFR in terms of population parameters or covariates is essential to understand the difference in CFR across different countries.
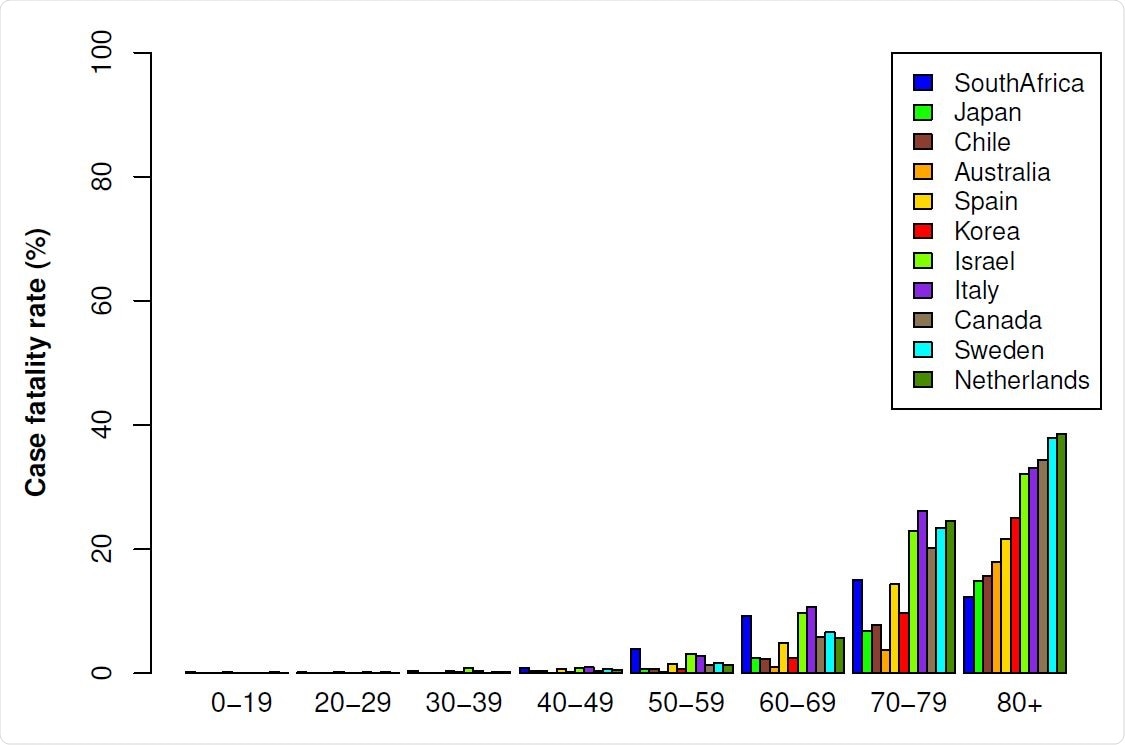
CFR by age groups for selected countries (as of 6 July 2020).
Analyzing CFRs at different times of snapshots during the first and second waves of pandemic in different countries
Researchers from the USA recently analyzed CFRs at two different images – July 6, during the first wave, and December 28, during the second wave of the pandemic. Age and GDP were the population parameters of primary interest in this study since it was found that there is a strong correlation between age, GDP, and mortality among COVID cases19. Both of these emergency covariates have been used as a surrogate for the quality and abundance of public health. Studies have shown that CFR for the elderly is high, while it is very low for younger people under 30 years. The review is published on the preprint server medRxiv*.

CFR scale by age groups for selected countries as of 6 July 2020.
The study found that there was an abstract difference in CFR by age groups across several countries, which was chosen mainly because of the availability of data and showed a fair distribution of all over the world. The researchers analyzed investigative data, which led to interesting results. They showed that the effect of age is clearly pronounced among different age groups, and this abstract index is almost independent across different countries and at different times during the pandemic.
“Singapore is a country that stands out that has seen CFR very low, due to higher than average middle age.”
A reversal of the parameters during the first and second waves may be due to the time delay in the quality and abundance of health care.
Analyzing the CFR for different countries using age and GDP as a surrogate for health care quality and abundance allowed the researchers to understand the responsibilities of age and GDP in the different CFRs across different countries. despite limitations in data accuracy. The results showed that the responsibilities of GDP and age were also surprising. During the first wave, age was a more important factor than GDP, while the importance declined through the second wave of the pandemic. According to the authors, this could be partially explained by the use of the time delay in the quality and abundance of public health.
“The effect of abstract age is largely independent across different age groups which is clearly presented on both data with a roughly the same approximate approximation. ”
* Important message
medRxiv publish preliminary scientific reports that are not peer-reviewed and, therefore, should not be seen as final, guiding health-related clinical / behavioral practice, or be treated as information established.