The COVID-19 pandemic caused by beta coronavirus has been termed as severe respiratory coronavirus syndrome 2 (SARS-CoV-2). This coronavirus causes severe respiratory syndrome that was first identified in Wuhan, China, in December 2019. This new zoonotic virus has taken the world’s attention, rapidly becoming a pandemic .
Clinically, COVID-19 (coronavirus disease 2019) is a heterogeneous disease. Symptoms range from cough, sore throat, fever, myalgia or arthralgia, fatigue, headache, gastrointestinal problems, loss of smell or taste, among fewer other symptoms.
Identification of the risk factors is essential for rapid diagnosis, better follow-up, and prognosis of patients with disease. Age and comorbidities (such as diabetes, hip tension, stroke, cancer, kidney disease, and high cholesterol) have been shown to be risk factors associated with mortality in COVID-19 disease.
A new study of laboratory results of COVID-19 patients reveals a strong risk association with hematologic values such as leukocytes and neutrophils.
To differentiate between patients with severe and uncomplicated COVID-19, researchers from Peru found prognostic signatures in the blood samples of COVID-19 patients. Virgilio E. Failoc-Rojas et al. study of laboratory results and clinical prognosis of COVID-19 patients from a hospital in Peruvian Amazon. The results of this interesting new study are published on the preprint server medRxiv *.
The researchers found that higher levels of leukocytes, neutrophils, low levels of lymphocytes, monocytes, and eosinophils were strongly associated with mortality.
“Parameters such as leukocytes and neutrophils were statistically significantly higher in patients who died.”
The study
The study group consisted of 127 patients hospitalized from a hospital in Ucayali (located in the Central Jungle, in eastern Peru). All patients were tested for COVID-19 in the period from March 13 to May 9, 2020. COVID-19 testing was confirmed through a polymerase reaction-transcriptase (RT-PCR) chain assay of nasopharyngeal swab samples and early immunochromatographic test. The population saw a mortality of 75 people.
Laboratory assays included leukocytes, neutrophils, platelets, RDW-SD (red cell circulation width with normal deviation), RN / L (neutrophil-lymphocyte ratio), fibrinogen, CRP (protein C -reactive), D-dimer, DHL (Lactate Dehydrogenase), hematocrit, monocytes, and eosinophils.
Although the study population had high levels of biochemical and hematological values, the researchers expressed specific observations according to mortality.
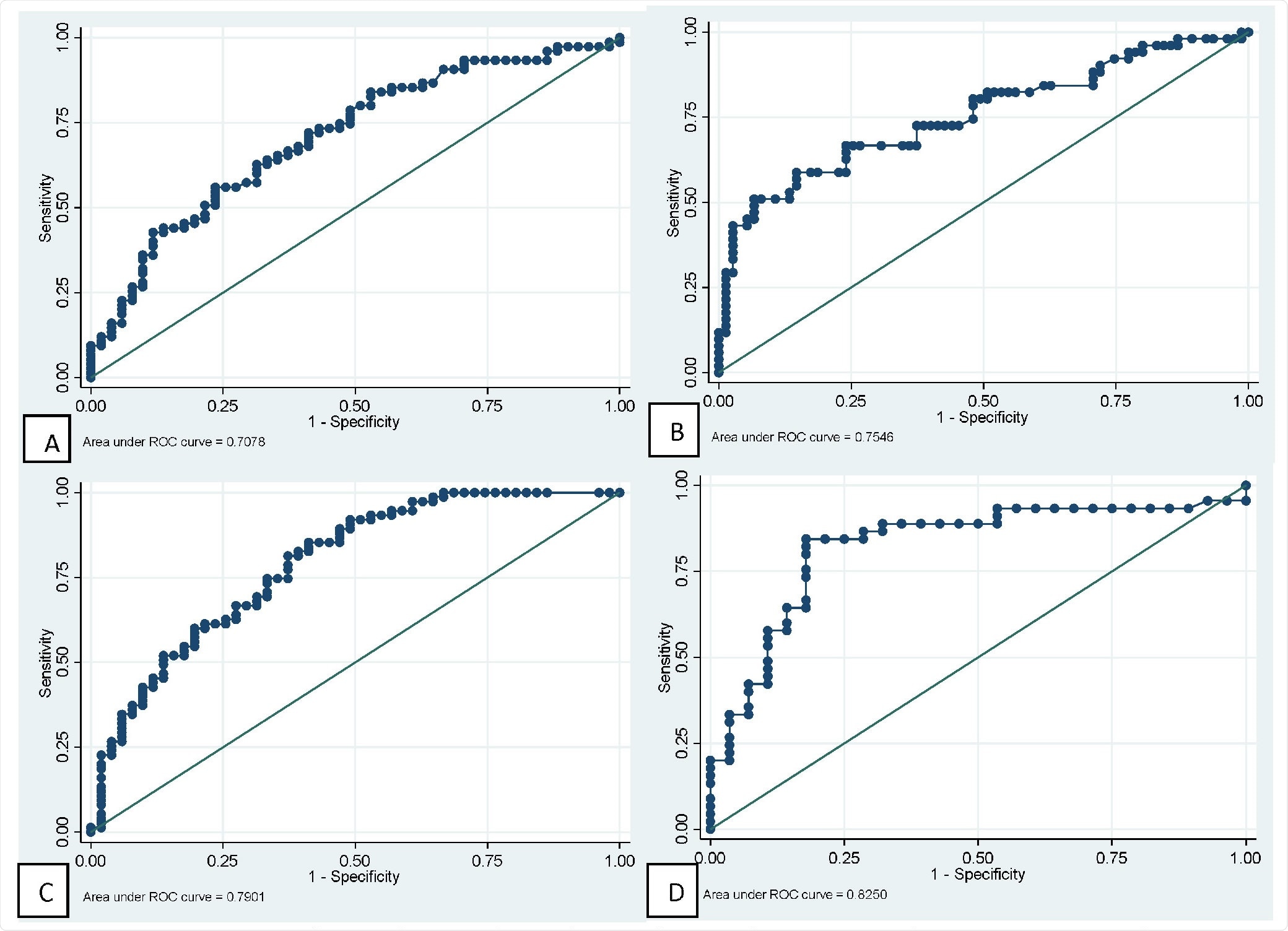
ROC curves of major hematological tests for predictive mortality in patients with COVID-19. A: Neutrophil. B: Lymphocytes. C: Neutrophil / lymphocyte ratio. D: Fibrinogen.
They found: 1) leukocytes and neutrophils were higher in patients who died 2) they also had lymphocytopenia (extremely low level of lymphocytes) compared to normal values in survivors (720 vs. 1,360 respectively), and 3) low levels of monocytes and eosinophils.
The researchers also found that other parameters such as the RN / L and fibrinogen were higher in the dying population than those that survived. The values are plate-like, red-cell circulating width with standard deviation (RDW-SD), and D-dimer, in each group.
Consistent with other studies, they found in this study that for every one-year increase in age, the probability of death increased by 4%.
IRR (Incident Risk Ratio) analysis for the numerical variables showed results that were strongly associated with hematological values such as Leukocytes (scale with 2,500 units), neutrophils (scale with 2,500 units); on the contrary, it is claimed that the increase of 1,000 units in lymphocytes, the probability of death down 48%, the researchers write.
In particular, the researchers found the most important link of a D-dimer with death. They found that high levels of D-dimer – for every 1 mg / L increase – increased the risk of death by 25%. D-dimer is a fibrin depletion product that exhibits hypercoagulability and thrombotic events.
Conclusion
To date, COVID-19 has claimed over 2.26 million lives out of more than 104 million confirmed COVID-19 infections worldwide. The observations from this study are important in understanding the prognosis of patients with COVID-19. This new information may help provide timely therapeutic support and enable patients ’condition to progress from normal to severe.
COVID-19 is known to have significant effects on the hematopoietic system and hemostasis; leukocytosis, lymphopenia, and thrombocytopenia are associated with increased severity and even death in COVID-19 cases. Prognostic lymphopenia may be considered.
This study looks at the biochemical and hematological parameters of COVID-19 patients in relation to mortality risk. Against this background, the researchers found various parameters that are strongly associated with death.
These observations in COVID-19 patients – hard and non-hard – will help to better understand the key features. Such a study, looking for prognostic indications for a variety of symptomatic diseases such as COVID-19, leads future disease study, control, and prevention.
* Important message
medRxiv publish preliminary scientific reports that are not peer-reviewed and, therefore, should not be seen as final, guiding health-related clinical practice / behavior, or be treated as information established.
Magazine Reference:
- Prognosis and hematological findings in patients with COVID-19 in the Amazonian population of Peru, Sebastian Iglesias-Osores, Arturo Rafael-Heredia, Eric Ricardo Rojas-Tello, Washington A. Ortiz-Uribe, Walter Leveau-Bartra, Orison Armando Leveau-Bartra, Miguel Alcantara-Mimbela, Lizbeth M. Cordova-Rojas, Elmer Lopez-Lopez, Virgilio E. Failoc-Rojas, medRxiv, 2021.01.31.21250859; doi: https://doi.org/10.1101/2021.01.31.21250859, https://www.medrxiv.org/content/10.1101/2021.01.31.21250859v1