A new study recently appeared on the preprint server medRxiv * makes use of an integrated method to estimate population exposure to true respiratory coronavirus 2 (SARS-CoV-2) syndrome, taking into account the fact that circulating antibodies to the virus will not be patients recovering from the disease. The scientists from Oxford University, UK and the University of Melbourne, Australia, concluded that the exposure could be twice as high, or even higher, than that found by seroprevalence studies in the UK.
The importance of serology
Serological studies help to understand the proportion of pathogen exposure in a population, which helps to identify at what point in epilepsy a particular region or country is. The reporting of cases in the 2019 pandemic of coronavirus infection (COVID-19) has been found to indicate only a fraction of the actual diseases. Thus, seroprevalence appears to be a more accurate method of assessing population exposure.
However, an important new performance has emerged, namely, the rapid reduction of specific antibodies against the virus to unrecognizable levels, or seroreversion. Researchers have found that antibody titers lower cellular immunity as indicators of long-term immunity, preventing relapse, but the latter are more difficult and expensive to quantify.
As a result, most countries still rely on seroprevalence studies, including England, which conducted one such study from 20 June to 13 July 2020. As a result there was a frequency of estimated disease 13% in London, and 6% in England, overall. . On this basis, the infectious mortality ratio (IFR) was calculated to 0.90%. The estimate did not take into account a decrease in antibody levels, which may have led to an underestimation of the actual infectious levels.
, and diagnosis (above the timeline) of diseases and overcoming. Levels marked in gray represent possible events, with a probability consistent with the darkness of a gray shadow.")
Progression of exposed individuals through the various clinical stages (below the timeline), and diagnosis (above the timeline) of diseases and overcoming. Levels marked in gray represent possible events, with a probability consistent with the darkness of a gray shadow.
Seroreversion affects seroprevalence
Continuous monitoring shows that antibodies are available for about six months after infection. Once they fall below the normal assay detection rate, the test is interpreted as negative. In other words, a negative serological test can indicate either the absence of antibodies or decay in antibody titers over time. This may be due to the fall in seroprevalence in England after the peak near the end of May 2020, rather than the steady increase expected as more people become infected over time. .
This seroreversion is defined as “within the mean time taken after seroconversion for antibody levels to fall below the cutoff level for seropositive testing.The extent of overexpression of the true magnitude of an epidemic may therefore depend on the time at which the serologic examination is ongoing, or in other words, the time elapsed since first peak of the disease.
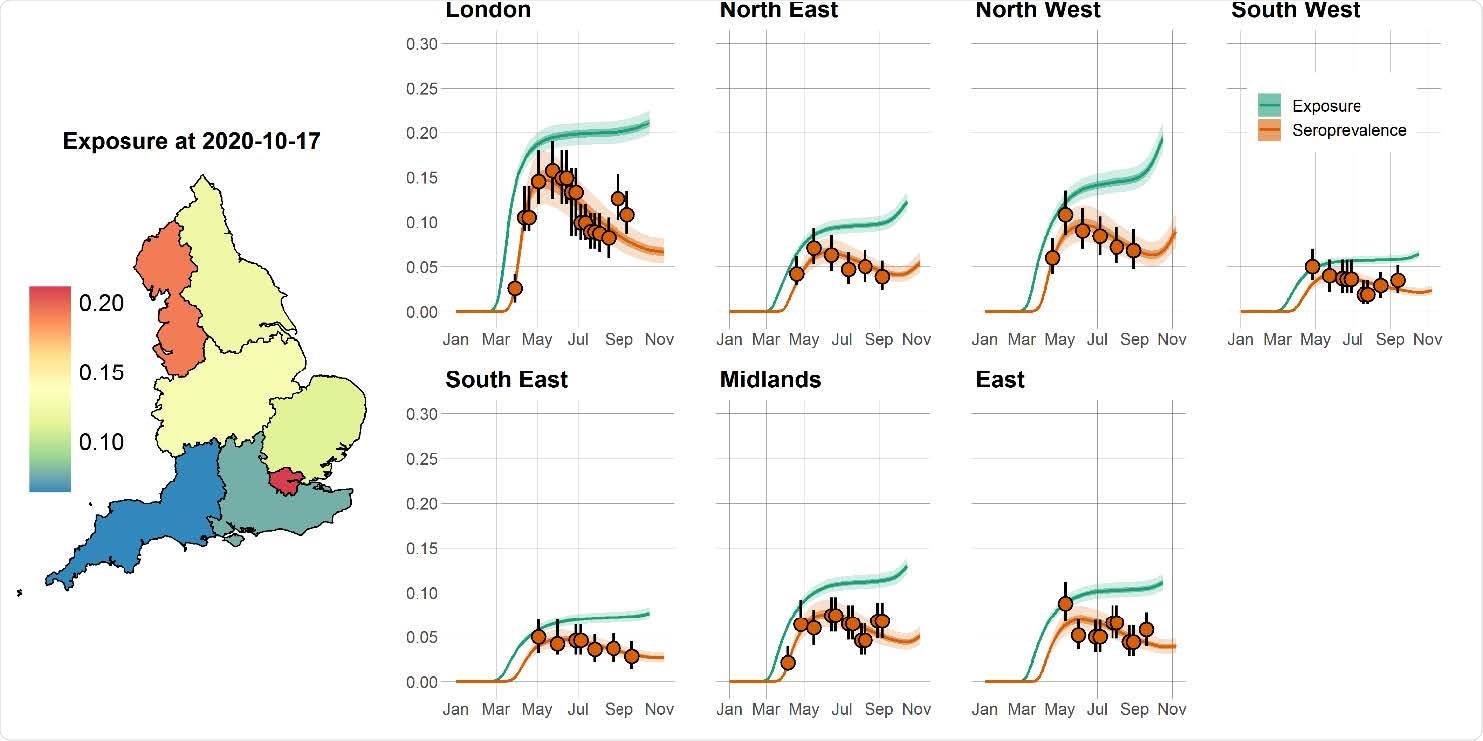
Time course of the SARS-CoV-2 pandemic up to 7 November 2020 for seven regions in England. The solid orange circles and black error bars in each regional panel represent the observed seroprevalence data and their confidence interval, respectively, after adjusting for the sensitivity and specificity of the antibody test. The green and orange lines show a predictable model of median and seroprevalence manifestations, respectively, while the shaded areas correspond to 95% CrI. The predicted regional prediction rates (expressed as the proportion of the population infected) from 17 October 2020 are shown on the map of England.
Correcting serology-based estimates
The current study suggests a data triangulation method to measure the number of people infected over time. The researchers used the mortality rate and seroconversion for this measure. The dates on which a specific death count could be used in relation to seropositivity were calculated according to the median time between infection and onset of symptoms, onset and symptom testing, and onset of symptoms to IgG production. This resulted in a period of 21 days from being seen with seroconversion, assuming antibodies lead to antibodies at the same time.
The method therefore targeted the IFR in different parts of England, such as the harbor variable, using this to detect the number of infected people at three weeks before the date of the measured IFR. This has been used by other scientific organizations, but the current study uses data at a regional level within a country, on the basis of data confirmed by another independent study conducted at the same time.
Diseases can be twice the number of seropositives
The results show that seroconversion is followed by seropositivity for about 161 days, after which they serve. This means that as the epilepsy progresses, the total population will move further away from the seroprevalence measurements. “Ultimately, this could mean that more than twice as many people have been exposed to the virus compared to the number of people who are seropositive.. ”If so, seroprevalence data would be an unreliable parameter on which to restrict policies.
Analysts also considered the nationwide variable IFR over time. This may be due to different age structures in the population in different parts of the country. On the other hand, this may be due to selection for the weakest sections of society as epilepsy progresses because in the first stage of the revolution, the weakest are more likely to die. So, over time, the IFR is likely to go down.
They found that the test confirmation ratio performs better than either case mortality ratio (CFR) or hospital mortality ratio (HFR), in terms of graph prediction. frequency of mortality. So they used these to find the time-changing IFR.
Viruses pick for people who are less vulnerable over time
The study shows that it is probably only London that has shown a significant difference in IFR with epidemic progression, which has declined sharply. This may be due to the pronounced age structure of the city, unlike other regions. Exposure levels do not appear to be driving this difference as forecast levels are similar to the North West of England but without a similar change in the IFR. Instead, younger numbers with fewer frail people show clear selection weight compared to other more mixed numbers.
What is the impact?
The researchers confirm that these findings do not mean that herd immunity cannot be achieved due to rapid seroreversion. The fact is that neutralizing antibodies do not equate to absolute antibodies, and an effective titer of the former may correspond to a degree of decay of the latter. Also, T cell immunity has been found in seronegative individuals and is protective against infection. This method is only useful for a reliable assessment of population frequency and thus may help to shape future restriction policies.
They also say that the study does not mean that herd protection is almost achieved in London because of its high level. Instead, this may be due to London having a higher proportion of younger people compared to the rest of England, which led to a higher original IFR due to bogus people complying with COVID. -19 at a higher level, and then fall as a result of selection processes.
Using this method that is based on seroprevalence but describes seroreversion, using mortality data, the researchers estimated that the actual population is cumulative in the seven regions they studied. double or greater than the estimate reached by seroprevalence studies, in particular, the REACT study. Such estimates would make it easier to evaluate the potential role of vaccines and other interventions in breaking the transmission chain in this pandemic.
* Important message
medRxiv publish preliminary scientific reports that are not peer-reviewed and, therefore, should not be seen as final, guiding health-related clinical practice / behavior, or be treated as information established.