At the onset of the 2019 coronavirus outbreak (COVID-19) the seventh known pathogenic human coronavirus, coronavirus-2 (SARS-CoV-2) inflammatory bowel syndrome.
Others include endemic seasonal human coronaviruses, HCoVs, including two alphacoronaviruses, 229E and NL63, and two beta coronaviruses, OC43 and HKU1 (all of which cause a common cold), respiratory coronavirus Syndrome Middle East (MERS-CoV), and Severe Respiratory Coronavirus Syndrome (SARS-CoV).
Chronic pandemic is the most pathogenic and widespread of these viruses, with more than 65 million registered diseases and more than 1.6 million deaths identified to date.
With no effective antiviral development to date, physicians have turned to a convalescent plasma (CP) test technique. Also, many monoclonal antibodies have been developed that target a specific epitope of the SARS-CoV-2 virus, to neutralize it. Early though, CP has received Emergency Use Authorization, and its benefit is backed by some initial data, especially when there are neutral high titers.
Antibody response to the polyclonal virus, with different patients exhibiting different titrations of antibody, is directed to different antigens, with different entry type, isotype use, and the self-defense provided by the antibodies.
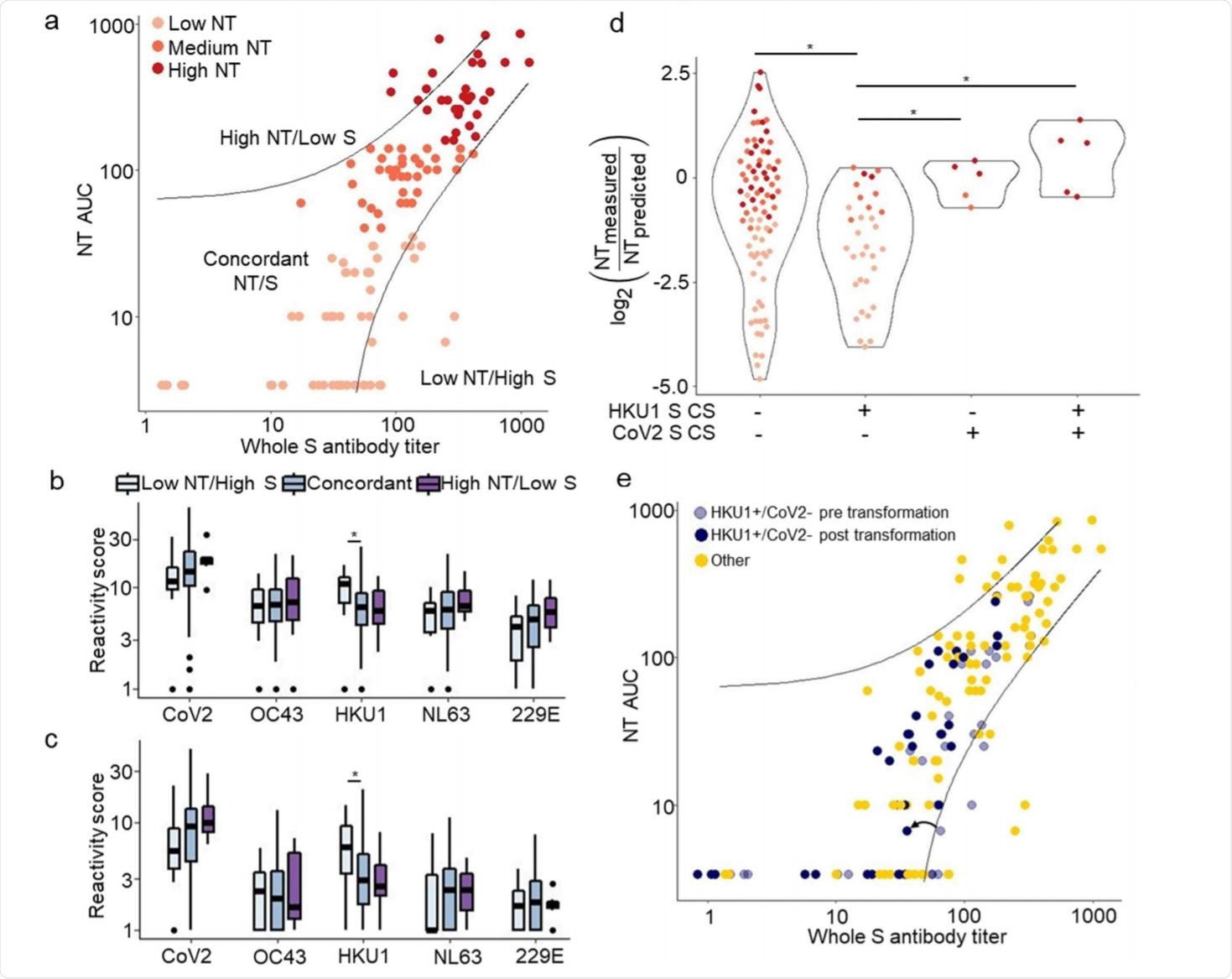
VirScan identifies discrepancy-related features between full spike titer and NT AUC. Image credit: https://www.medrxiv.org/content/10.1101/2020.12.16.20248294v1.full.pdf
Original antigenic sin
Previous antibodies directed against SARS-CoV-2 spike protein are present in a small percentage of the population. This may be due to the highly conserved nature of the sequences encoding the S2 viral subunit, which are essential for the entry of virus into the host cells.
Due to the shared nature of these sequences, titers of such antibodies may arise in response to SARS-CoV-2 infection, without benefit to the patient in terms of neutralizing potency or immunity. against the virus. Canar ‘original antigenic sin,”Where the immune response against a pathogen or antigen mainly involves antibodies or T cells formed when they appeared earlier on a related pathogen or antigen.
Study aim and details
The current study aimed to examine the notion that this variant is confirmed by the existing antibodies induced by endemic HCoVs. The researchers used systemic serologic tests and fully complex epitope analysis, to determine the functional properties of CP, as well as the exact epitopes associated with different CoV antibodies. Their research was published in the preprint server medRxiv *.
They studied the antibodies in CP donated by 128 donors, at intervals of 13–67 days after detection of COVID-19 by reverse-transcriptase polymerase chain reaction (RT-PCR). The CP was assigned for use in a clinical trial, so the titer of neutralizing antibodies (titrating neutralizing, NT) was measured for each sample.
The researchers classified the CP into high, medium, and low NT samples, where the area was below the curve for NT 160 or higher, 40–159, and less than 40, respectively. They also measured other functional characteristics, namely, antibody-dependent cellular phagocytosis (ADCP), antibody-dependent cellular cytotoxicity (ADCC), and antibody-dependent filler deposition (ADCD). for each sample.
VirScan Library
They used a large library of more than 3,400 peptide epitopes, all 56 residues in length, from a range of 230 COVID-19 samples and 190 premature samples starting COVID-19. This was prepared using a complex antibody profile system, VirScan, which studied very large numbers of epitopes simultaneously. The library covers the seven human pathogenic coronaviruses, as well as three associated bat coronaviruses.
Using the VirScan library, the researchers were able to identify the epitopes in each sample, while also comparing 87 samples from the time of the pandemic. Any area that showed 20% was thought to be binding with a reactive antibody. This turned up 27 domains of dominant reactivity, mostly corresponding to regions already known.
The NT AUC was not associated with the reactivity rate of these regions to specific peptides, with the exception of one area that crossed the spike-binding domain (RBD) of the SARS-CoV-2 . This area was more reactive in the high NT group.
This indicates that, with individual peptides, the number of reactive epitopes is more important than the amount of binding with individual peptides in differentiating low NT from high NT CP. With high NT samples, in 50% to 100% of cases, antibodies target three segments of the Spike protein (S), one segment of the membrane protein (M), and four of the nucleocapsid protein (N).
With moderate NT and low CP, lower recognition frequency was observed. However, the researchers found that low NT plasma was largely reactive to S1 / S2 (CS) acting site peptides from the seasonal beta coronaviruses.
High reactivity associated with high NT
High NT CP was associated with the highest reactivity for SARS-CoV-2 proteins, but also higher total reactivity of NL63 and OC43, which indicates cross-reactivity. The greater the number of SARS-CoV-2 and NL63 regional epitopes that showed reactivity with the CP, the higher the NT AUC.
Fusion peptides of the epitopes are highly concentrated
Many of the major HCoV regions were found to exhibit increased NT AUC-related reactivity, such as the spike fusion peptide required for cell entry. In public databases of SARS-CoV-2 proteins, this category is among the most targeted epitopes, with a high sequence distribution among the HCoVs. As a result, these epitopes cause an increase in cross-reactive HCoV / SARS-CoV-2 antibodies after infection with the latter.
Overall, the fusion peptides of the S2 subunit of the HCoVs and SARS-CoV-2 were the most reactive among the NT groups for all coronavirus. Again, plasma treated with the fusion peptide SARS-CoV-2 was more likely to respond with all other CoV fusion peptides. Even in pre-pandemic plasma samples, cross-reactivity was 8% with fusion peptide and HR2 peptide from SARS-CoV-2.
Peptides treated in the NT AUC were also associated with other functional properties of CP, as would be expected from their independent correlation.
High NT plasma detection
Enhanced CP is characterized by antibodies generated by multiple B cells, in response to multiple epitopes of SARS-CoV-2 and NL63, and by cross-reactivity to peptide fusion of their precursors. When only HKU1 (CS) acting site peptides were identified, but not the CS peptides of SARS-CoV-2, neutralization activity was significantly lower compared to high NT CP. On the other hand, reactive antibodies for SARS-CoV-2 RBD rather than for HKU1 RBD bind to high NT plasma.
Thus, the highly polyclonal nature of SARS-CoV-2 antibody responses explains a highly neutral response.
Individual reactivity predicts high NT
The peptide-antibody binding that tended to be associated with ADCC was from a component of the M-region that activates T cell binding. Other CP potentials, such as ADCC, ADCP, and ADCD, are linked. Individual reactivation of each peptide may bind to fully activated CP in one of two ways.
First, the worse the disease, the higher the NT, which may be reflected in an individual increase in relapse. On the other hand, the greater the reactivity, the more effective the antibody response may be, and therefore, the more severe the disease.
What is the impact?
The researchers suggest that much of the reactivity to HCoV peptides present in CP is due to an increase in pre-existing HCoV antibodies to the SARS-CoV-2 infection – also known as reaction anamnestic – or as a result of cross-reactivity itself. Thus, these HCoV antibodies may be useful as biomarkers, helping to identify plasma strength.
In addition, their connection to a higher NT could reflect their protective role. The researchers maintained that neutralization activity is more closely related to the antibodies targeting the RBD, fusion peptide, and the peptide CS. The latter appear to be important in neutralization, as therapeutic antibodies have induced escape mutations in this region. Further study may reveal the interactions between anti-CS antibodies and the severity of COVID-19.
However, their analysis also showed that a stronger immune response to NL63 is associated with a stronger neutral response, as supported by earlier studies of milder disease by neutralizing antibodies to NL63. This may be due to the fact that both this virus and SARS-CoV-2 use the ACE2 receptor.
The immunosuppressive nature of cross-functional anti-HCoV / SARS-CoV-2 fusion peptides may support plasma storage stored in blood clots, containing anti-fusion peptide antibodies, in future revolution caused by coronaviruses.
As CP comes into wider use, plasma reactivation to HKU1 CS is a marker that may help identify plasma with high NT.
An understanding of the detailed specifications of anti-coronavirus antibody repertoires can be applied to therapeutic plasma priming. ”
The method described here may differentiate epitope-recognizing antibodies from nonspecific overreactivity, it may help to differentiate original antigenic sinus vs. heterologous protective antibodies for viruses other as well, and to differentiate antibody responses to closely related viruses.
* Important message
medRxiv publish preliminary scientific reports that are not peer-reviewed and, therefore, should not be seen as final, guiding health-related clinical / behavioral practice, or be treated as information established.